Takayasu arteritis: 18F-FDG-PET/CT
Figure 1. CECT examination performed in a 37 year-old woman, admitted for suspected ascending aorta ectasia suitable for surgery. Axial (a, c, d) and coronal (b) CECT images show homogeneous low density thickening of aortic wall, mainly in the ascending-aortic tract (blue arrows, a and b) and to a lesser degree in the descending portion (blue arrow, d). There is also involvement of the origin of the main supra-aortic branches (wall thickness 4 mm, b). All the involved vessels demonstrate homogeneous caliper and opacification; no intraluminal flaps or parietal thrombi are present.
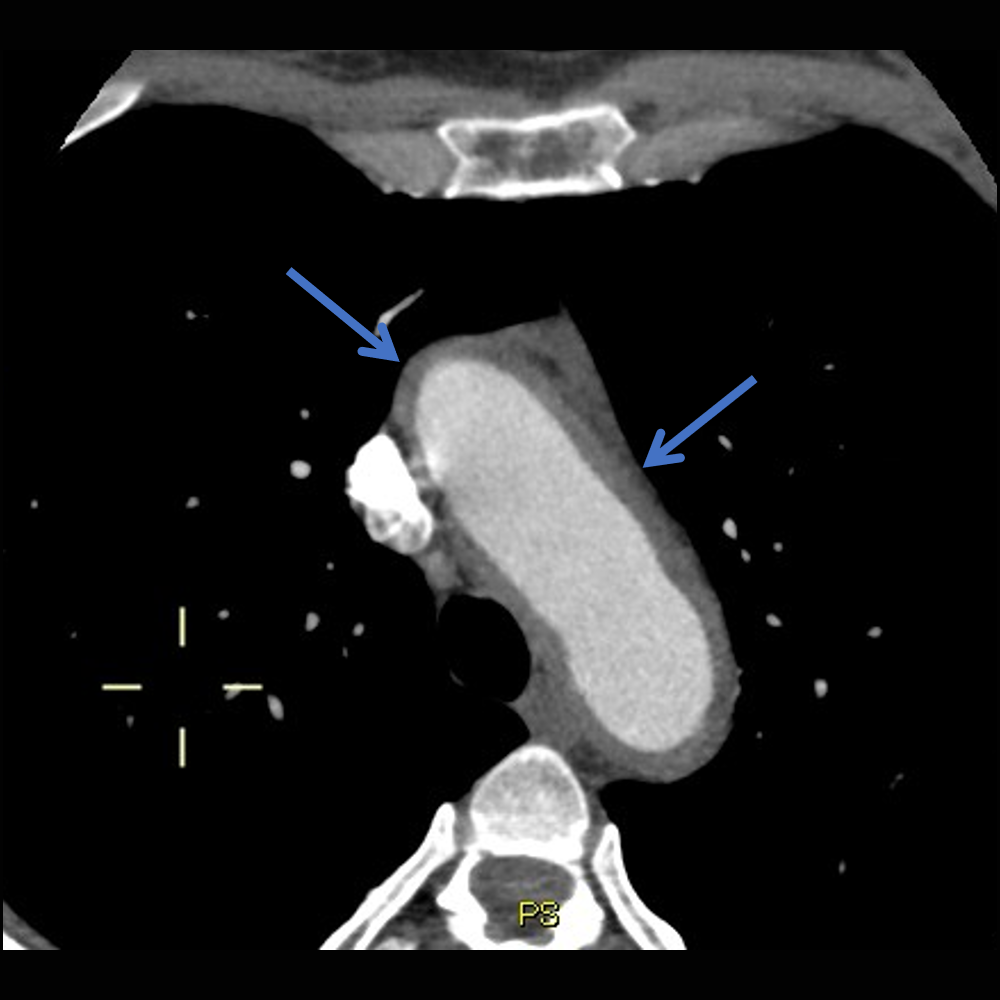
Fig. 1a
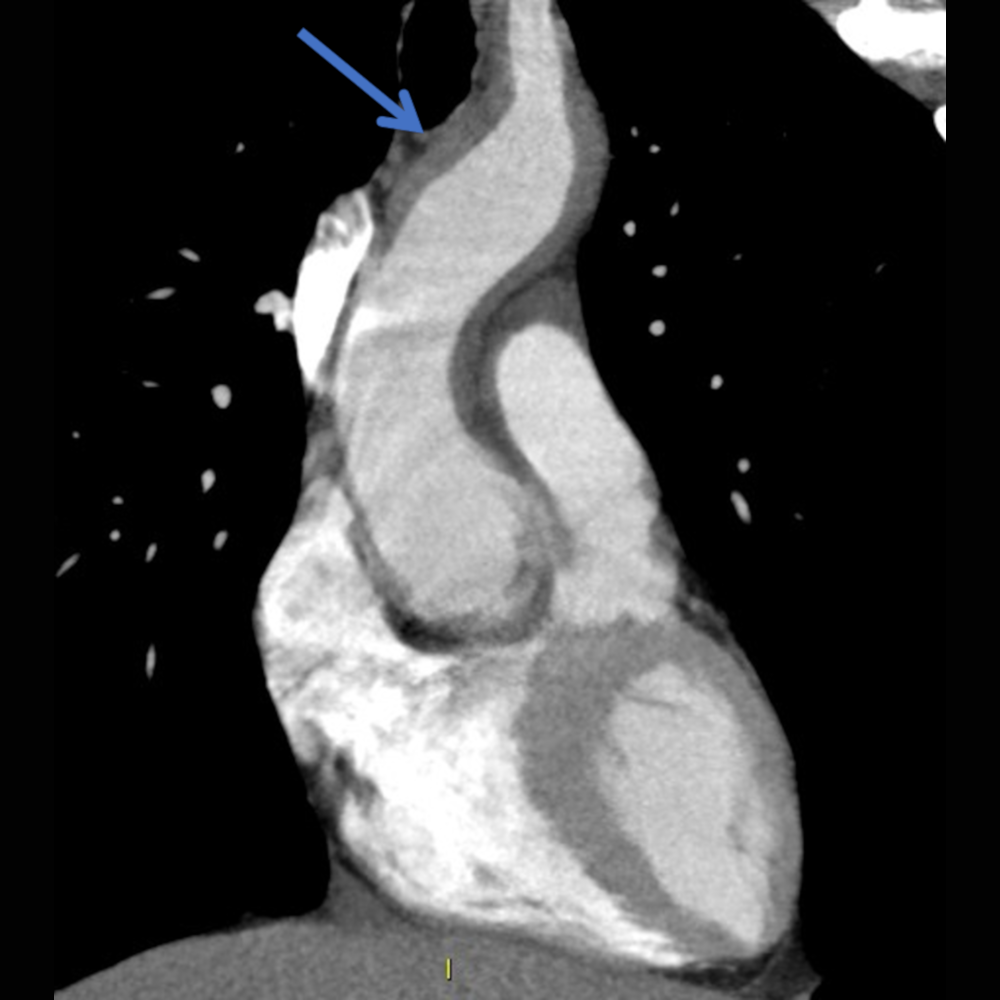
Fig. 1b
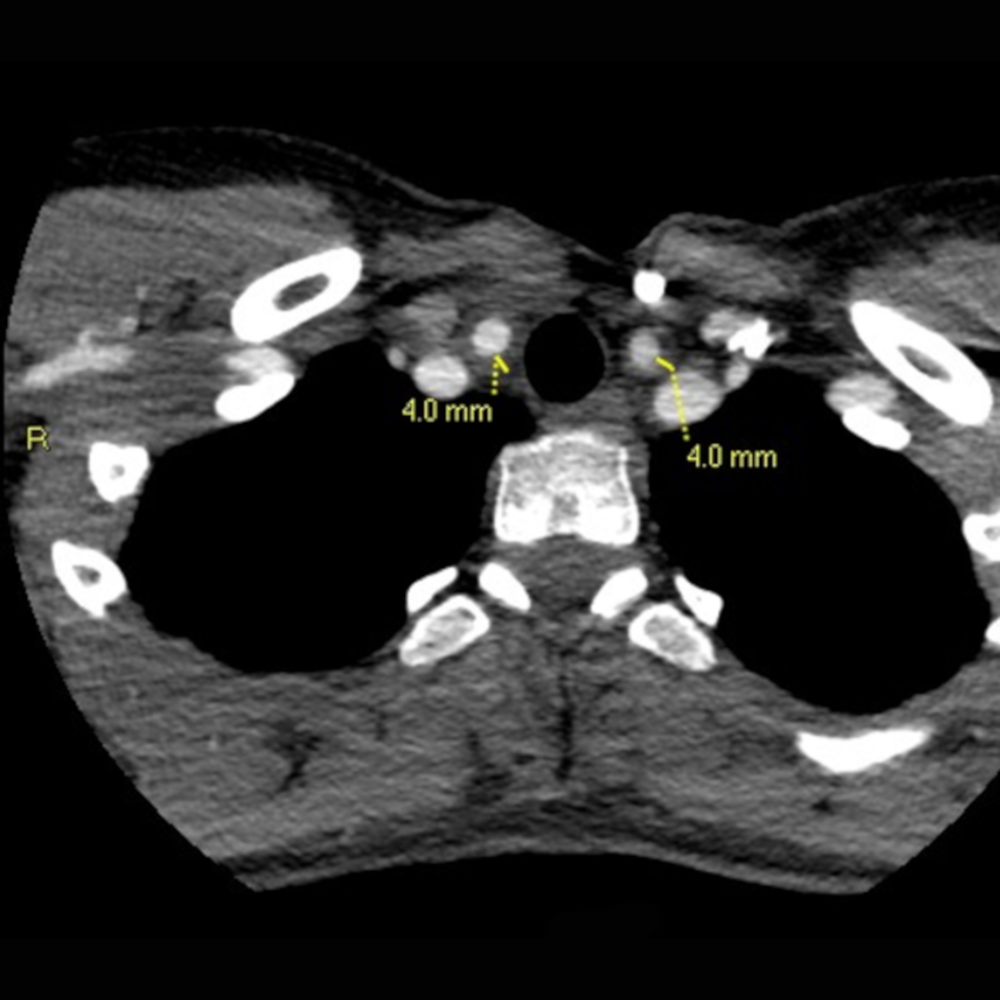
Fig. 1c
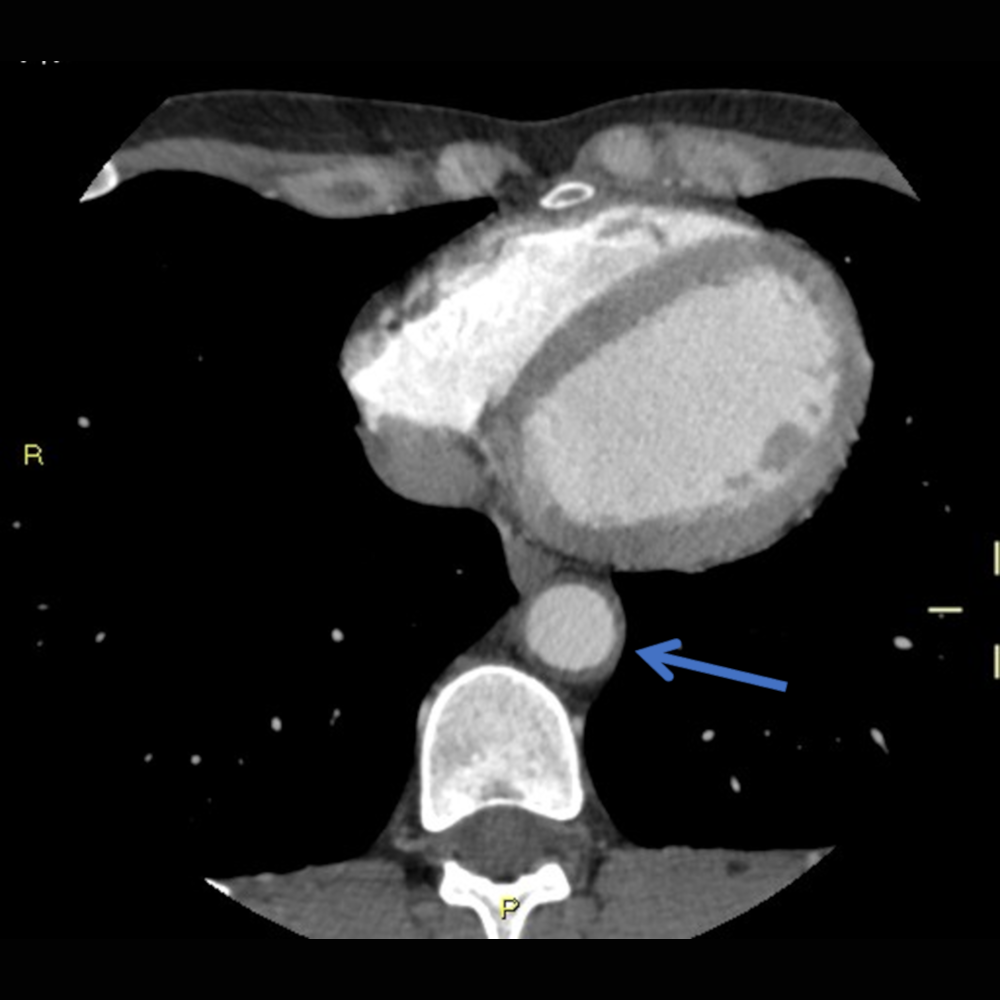
Fig. 1d
Figure 2. 18F-FDG-PET/CT study (a, b). Axial and coronal 18F-FDG-PET image show increased FDG uptake at the level of the aortic arch (blue arrows, a and b) and all along the ascending tract (curved arrow, b). There is also evidence of involvement of the origin of the supra-aortic branches (white arrowhead, b). The areas of increased uptake correspond to the arterial wall thickening highlighted by the baseline CT (Figure 1).
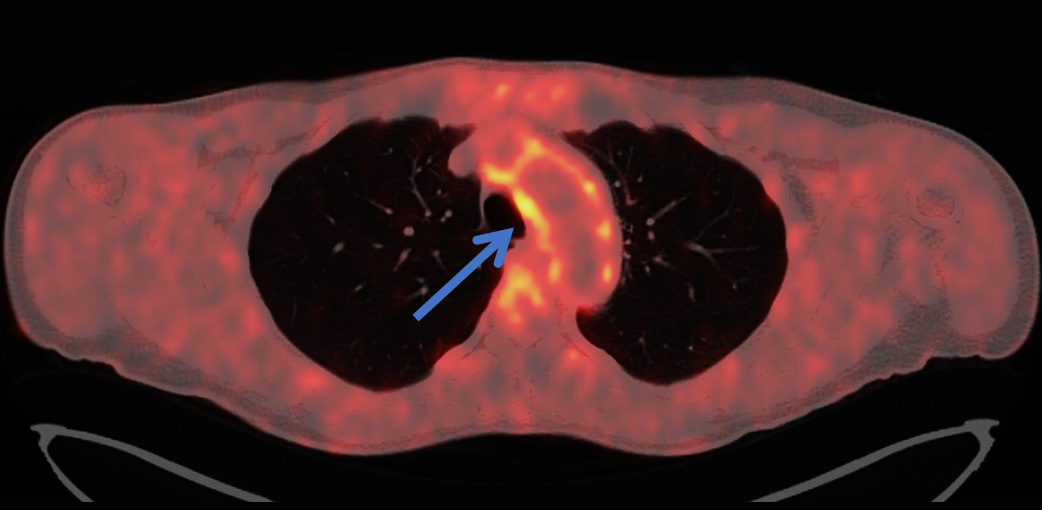
Fig. 2a
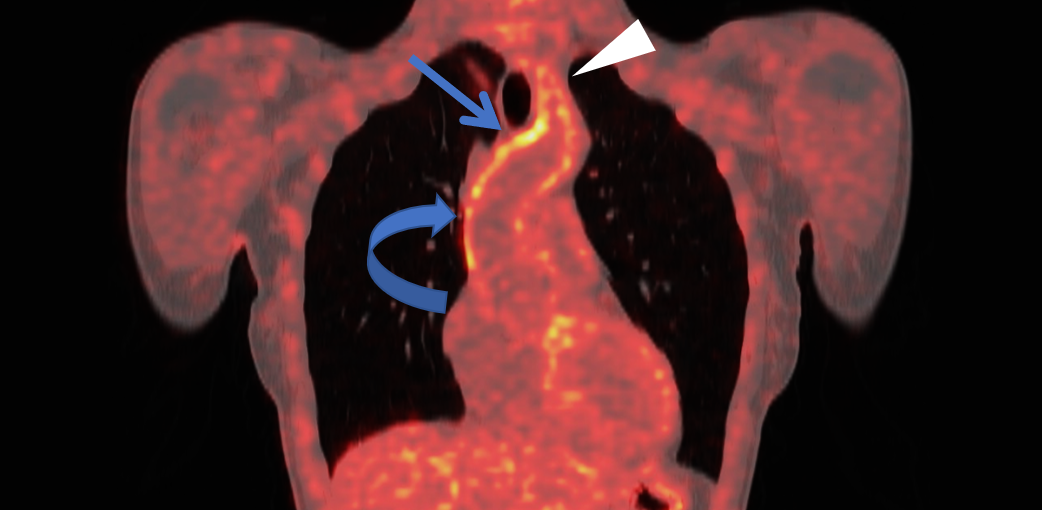
Fig. 2b
Summary:
Takayasu arteritis (TA) is a chronic granulomatous large vessel vasculitis, predominantly affecting the aorta (from ascending to abdominal tract) and its major branches. Pulmonary arteries can also be affected. Panarteritis can involve all arterial wall layers, progressing to thickening and stenosis.
The etiology is not well known. Immune system abnormalities are thought to be involved in triggering inflammatory changes.
TA has a strong predominance in females <50 years of age (typical onset 15-30 years) and increased prevalence in Asian populations.
Clinical presentation includes: non-specific systemic symptoms (illness, fever, myalgia; rarely as FUO), ischemic symptoms (narrowing, stenosis, thrombus formation), aneurysm formation.
CT represents the mainstay in diagnosis and main findings include: wall thickening and enhancement, possible aortic valve disease (stenosis, regurgitation), major branches occlusion or late distal narrowing, aortic/major branches aneurysm.
PET can estimate the degree as well the site of inflammation and has been reported to be more reliable than MRI for monitoring disease activity during therapy. Moreover, SUVmax increases as inflammatory reaction spread, serving therefore as quantitative marker of disease activity.
This Case was kindly provided by:
Dr. Valle Clarissa (staff)
Post Graduate School of Diagnostic Radiology, University of Milano-Bicocca
Department of Radiology, ASST Papa Giovanni XXIII Hospital
Piazza OMS 1, 24127, Bergamo – Italy
Dr. Bonaffini Pietro Andrea (staff)
Post Graduate School of Diagnostic Radiology, University of Milano-Bicocca
Department of Radiology, ASST Papa Giovanni XXIII Hospital
Piazza OMS 1, 24127, Bergamo – Italy
Prof. Sironi Sandro (chief)
Post Graduate School of Diagnostic Radiology, University of Milano-Bicocca
Department of Radiology, ASST Papa Giovanni XXIII Hospital
Piazza OMS 1, 24127, Bergamo – Italy